QUICK FACTS
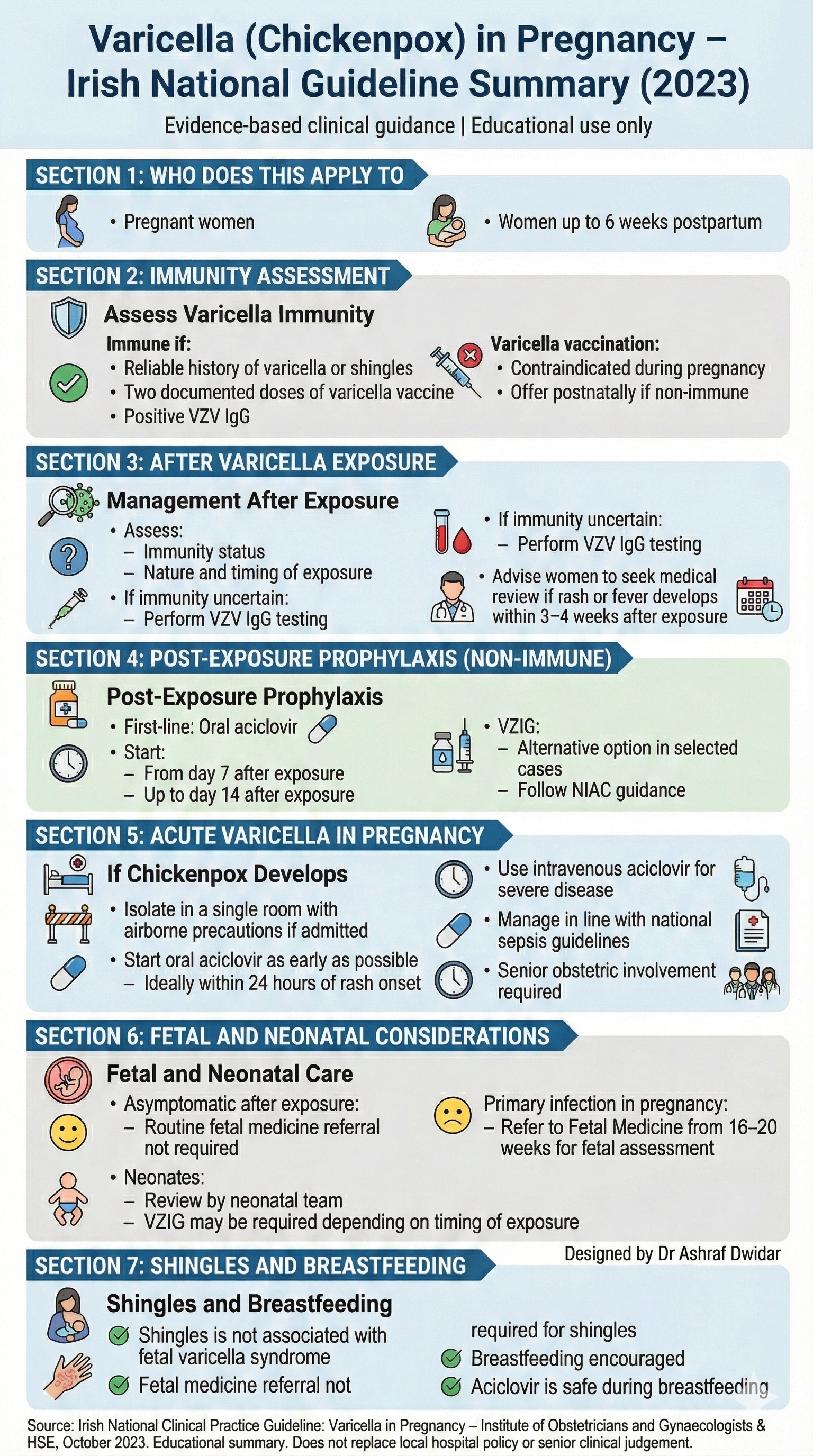
Varicella (Chickenpox) in Pregnancy
Irish Guideline
-
Pregnant women
Women up to 6 weeks after delivery
Based on the Irish National Clinical Guideline (2023).
Educational summary only — follow local hospital policy.
-
Check immunity at booking
Immune if:
Previous chickenpox or shingles
Two doses of varicella vaccine
Positive VZV IgG
Varicella vaccine:
Not given in pregnancy
Offered after delivery if non-immune
-
Assess:
Immunity status
Type and timing of exposure
If immunity unclear:
Check VZV IgG
Advise review if rash or fever develops within 3–4 weeks
-
Oral aciclovir is first choice
Start:
Day 7 after exposure
Up to day 14
VZIG may be used in selected cases
-
Isolate if admitted
Start aciclovir early
Use IV aciclovir for severe disease
Involve senior obstetric team
-
Routine fetal review not needed if mother asymptomatic
Refer to Fetal Medicine if infection occurs in pregnancy
Shingles is not linked to fetal varicella syndrome
Breastfeeding is safe
Aciclovir is safe during breastfeeding
-
Irish National Clinical Practice Guideline:
Varicella in Pregnancy – HSE & IOG, October 2023.
Post-exposure prophylaxis for pregnant women exposed to VZV
Click through the pathway. This is an educational decision aid — always follow your local hospital policy and the guideline version in use.
- Aciclovir 800 mg four times daily for 7 days.
- Start on day 7 after exposure (can be started up to day 14).
- VZIG can be used as an alternative if required (per local policy).